Renal Physiology
Return to the Main Menu
Case 1:
(Click here to go to the answers)
A 68-year-old woman has had increasing malaise for the past 6 years. On physical examination, vital signs include temperature 36.9 C, pulse 77/min, respiratory rate 16/min, and blood pressure 165/100 mm Hg. Laboratory studies show sodium 143 mmol/L, potassium 4.2 mmol/L, chloride 108 mmol/L, CO2 27 mmol/L, glucose 109 mg/dL, and urea nitrogen 40 mg/dL.
A 24 hour urine collection is performed.. There are 0.9 g of creatinine in 860 mL of urine. Her serum creatinine is 3.6 mg/dL.
Questions:
1.1 Calculate her creatinine clearance.
Urine creatinine x Urine volume in ml
Creatinine clearance = --------------------------------------
Plasma creatinine x time in min
A "corrected" creatinine clearance can be calculated by multiplying by 1.73/total body surface area.
1.2 What does this indicate?
1.3 What pharmacologic therapy is indicated?
1.4 If she is receiving amoxicillin, how should the dose be adjusted?
Case 2:
(Click here to go to the answers)
A 44-year-old man participates in a health screening program and is found to have a blood pressure of 166/106 mm Hg. He goes to a physician who finds no abnormalities on physical examination. Laboratory studies show sodium 140 mmol/L, potassium 3.9 mmol/L, chloride 104 mmol/L, CO2 25 mmol/L, glucose 93 mg/dL, creatinine 1.4 mg/dL and urea nitrogen 32 mg/dL. A urinalysis shows pH 6.5 with sp gr 1.018, and no blood, protein, glucose, or ketones. Urine electrolytes show sodium 15 meq/L and osmolality 600 mosm/L.

An abdominal ultrasound shows normal sized kidneys without dilation. The length between the markers is about 12 cm.
He is placed on an angiotensin converting enzyme (ACE) inhibitor. A week later he develops increasing nausea, headache, and oliguria. He takes ibuprofen for the headaches. His condition does not improve.
Below is a normal renal scan, with intravenous administration of Tc-99m (a radionucleide), following by timed images.
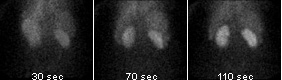
In the following study, the patient had a renal scan performed priorto administration of intravenous enalapril:
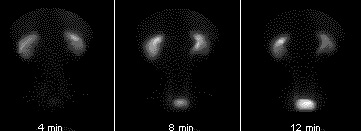
In the following study, the patient had a renal scan performed after administration of intravenous enalapril:
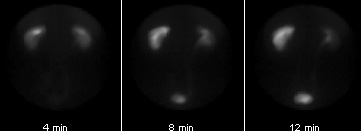
Following administration of the ACE inhibitor, there is marked asymmetry in renal function, with normal uptake and excretion by the right kidney but little or no excretion on the left. This test is a good screening tool for renovascular hypertension.
Another study is performed, as shown below:

Questions:
2.1 Explain what may have happened?
2.2 Explain the progression of his disease?
2.3 What pharmacologic therapy should he have initially received?
2.4 What can be done next?
Case 3:
(Click here to go to the answers)
A 72-year-old man working on the roof of his house falls about 4 m to the ground. He is taken to the local emergency department. On physical examination vital signs show T 37 C, P 70/min, RR 17/min, and BP 140/90 mm Hg. There is a 4 cm contusion with swelling over the left parietal region scalp. There is no papilledema. A head CT scan shows no intracranial hemorrhage or midline shift. He remains in stable condition. Over the next week he develops increasing polydipsia and polyuria.
Questions:
3.1 What is suggested by these findings? What additional diagnostic findings should be sought?
3.2 What is the most likely diagnosis?
3.3 What is his free water clearance, if his urine flow is 16 mL/min?
C of H2O = urine flow rate - ((urine osmolality / plasma osmolality) X urine flow rate)
3.4 What are normal body fluid compartments?
Case 4:
(Click here to go to the answers)
A 76-year-old woman with a history of essential hypertension has become increasingly lethargic with nausea and loss of appetite over the past week. On physical examination her vital signs show T 37 C, P 86/min, RR 23/min, and BP 120/70 mm Hg. There are no abnormal findings. Laboratory studies show sodium 131 mmol/L, potassium 5.3 mmol/L, chloride 93 mmol/L, CO2 12 mmol/L, glucose 63 mg/dL, creatinine 1.2 mg/dL, and urea nitrogen 18 mg/dL. An arterial blood gas shows pH 7.3, pCO2 30 mm Hg, pO2 84 mm Hg, and HCO3 13 meq/L.
Questions:
4.1 What is suggested by these findings?
4.2 What may be causing these findings? Describe the pathophysiology.
Case 5:
(Click here to go to the answers)
A 58-year-old man has a sudden fall to the ground. 911 is called and paramedics arrive 4 minutes later while his business associates attempt CPR. The paramedics confirm that he is in cardiac arrest. A cardiac rhythm is established, but his blood pressure is 70/40 mm Hg with pulse 109/min and irregular.
Questions:
5.1 What do you suspect? What tests would you perform?
5.2 How should he be treated at this point?
Additional history:
He is in unstable condition. His blood pressure varies from 90/60 to 70/palpable. Two days later his urine output drops. Laboratory studies show sodium 141 mmol/L, potassium 3.9 mmol/L, chloride 96 mmol/L, CO2 15 mmol/L, glucose 75 mg/dL, creatinine 2.4 mg/dL, and urea nitrogen 52 mg/dL. His fractional excretion of sodium is <1% while his urine osmolality is 550 mosm/mL.
5.3 What do these findings suggest?
Case 6:
(Click here to go to the answers)
A 59-year-old woman comes to her physician because she has been bothered by increasing swelling of her lower legs for the past 7 months. On examination her pulse is 80/min with blood pressure 140/85 mm Hg. Her lungs have a few fine basilar crackles on auscultation, and her heart rate is regular with no murmurs. She has 1+ pitting edema to her mid-calf bilaterally. A chest radiograph shows an enlarged heart with blunting of costophrenic angles. Laboratory studies show sodium 144 mmol/L, potassium 4.2 mmol/L, chloride 108 mmol/L, CO2 26 mmol/L, glucose 89 mg/dL, creatinine 1.0 mg/dL, and urea nitrogen 15 mg/dL. A fasting lipid profile shows total cholesterol 223 mg/dL, HDL cholesterol 28 mg/dL, and triglyceride 177 mg/dL.
Questions:
6.1 How do you interpret these findings?
6.2 What pharmacologic therapy is indicated?
6.3 How does this therapy work? Explain the pathophysiology.
Additional history:
A year later she comes back to the physician. Though she had some relief from the ankle swelling, she now has orthopnea. On physical examination her pulse is 87/min and blood pressure 130/80 mm Hg. She has diffuse crackles in all lung fields. Laboratory studies show sodium 135 mg/dL, potassium 3.7 mg/dL, chloride 92 mg/dL, CO2 24 mg/dL, glucose 80 mg/dL, and creatinine 1.1 mg/dL.
6.4 What pharmacologic therapy may be useful now?
Case 7:
(Click here to go to the answers)
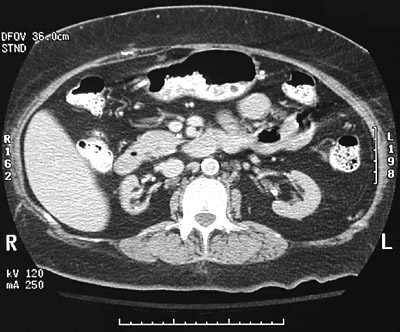
A 52-year-old man has developed polydipsia and polyuria over the past 4 months. On examination he is afebrile with pulse 79/min, respiratory rate 18/min, and blood pressure 160/95 mm Hg. On physical examination his liver span is increased. A chest radiograph shows a slightly enlarged heart with prominent left heart border. Laboratory studies show sodium 140 mmol/L, potassium 4.5 mg/dL, chloride 99 mmol/L, CO2 25 mmol/L, glucose 70 mg/dL, calcium 8.1 mg/dL, phosphorus 4.1 mg/dL, creatinine 3.5 mg/dL, and urea nitrogen 40 mg/dL. A urinalysis shows pH 6.5, sp gr 1.010, and no blood, protein, or glucose. The urine microscopic examination shows many oxalate crystals.
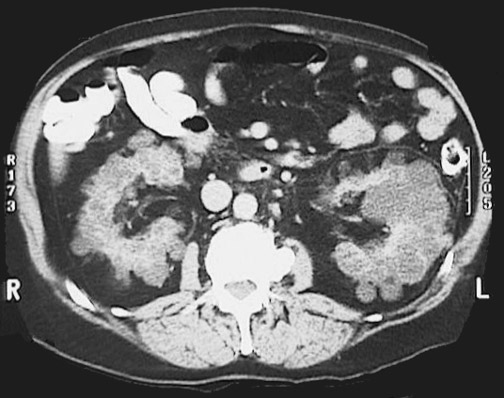
An abdominal CT shows markedly enlarged cystic kidneys bilaterally.
Questions:
7.1 What is suggested by these findings?
7.2 What pharmacologic therapy is indicated?
Additional history:
Three years later, he has increasing malaise and decreasing urine volume. Laboratory studies show his serum creatinine is 5.6 mg/dL and urea nitrogen 68 mg/dL.
7.3 What should be done at this point?
7.4 The patient is a jazz musician with no immediate family who travels frequently and whose income is quite variable through performances and CD sales. He wants to know how he will continue to receive treatment.
7.5 How is drug therapy now affected?
Case 8:
(Click here to go to the answers)
Adapted from: N Engl J Med 1995; 332:1038-1039
On April 13, 1945, the world learned of the sudden and unexpected death of Franklin D. Roosevelt, 32nd president of the United States, who had died in Warm Springs, Georgia, the day before. No one suspected that he had a serious medical condition, and Admiral Ross McIntire, the president's personal physician, stated that the fatal cerebral hemorrhage "came out of the clear sky". The pertinent findings as recorded by the president's cardiologist, Dr. Bruenn, are shown below:
At the start of the above chart, in March 1944, FDR had left ventricular hypertrophy on an EKG and cardiomegaly on chest x-ray. A urinalysis showed mild proteinuria. Throughout 1944 he had dyspnea from congestive heart failure.
On the morning of April 12, 1945, FDR reported a "terrific" occipital headache while being sketched for a portrait. He lost consciousness immediately thereafter and Dr. Bruenn recorded a blood pressure of >300/190 mm Hg. FDR was pronounced dead at 3:35 p.m. The president's medical record kept in a safe at the U.S. Naval Hospital in Bethesda, Maryland disappeared after his death and was never found again.
8.1 What is the diagnosis?
8.2 What was the consequence for world history?
8.3 What treatment is now available for this condition?
8.4 If his spot urine sodium was 10 meq/L, his serum sodium 140 meq/L, his urine creatinine 20 mg/dL, his serum creatinine 2 mg/dL, and his serum urea nitrogen 40 mg/dL, what would be the fractional excretion of sodium, and what would this indicate?
Urine sodium in meq/L x Plasma creatinine in mg/dL
Fe[Na] = -------------------------------------------------- X 100
Plasma sodium in meq/L x Urine creatinine in mg/dL
8.5 If his spot urine urine sodium was 40 meq/L, his serum sodium 140 meq/L, his urine creatinine 40 mg/dL, his serum creatinine 2.8 mg/dL, and his serum urea nitrogen 40 mg/dL, what would be the fractional excretion of sodium, and what would this indicate?
Urine sodium in meq/L x Plasma creatinine in mg/dL
Fe[Na] = -------------------------------------------------- X 100
Plasma sodium in meq/L x Urine creatinine in mg/dL
8.6 If his ekg had shown the following, what would you do?

Return to the Main Menu
|