|
A 52-year-old man has developed polydipsia and polyuria over the past 4 months. On examination he is afebrile with pulse 79/min, respiratory rate 18/min, and blood pressure 160/95 mm Hg. On physical examination his liver span is increased. A chest radiograph shows a slightly enlarged heart with prominent left heart border. Laboratory studies show sodium 140 mmol/L, potassium 4.5 mg/dL, chloride 99 mmol/L, CO2 25 mmol/L, glucose 70 mg/dL, calcium 8.1 mg/dL, phosphorus 4.1 mg/dL, creatinine 3.5 mg/dL, and urea nitrogen 40 mg/dL. A urinalysis shows pH 6.5, sp gr 1.010, and no blood, protein, or glucose. The urine microscopic examination shows many oxalate crystals.
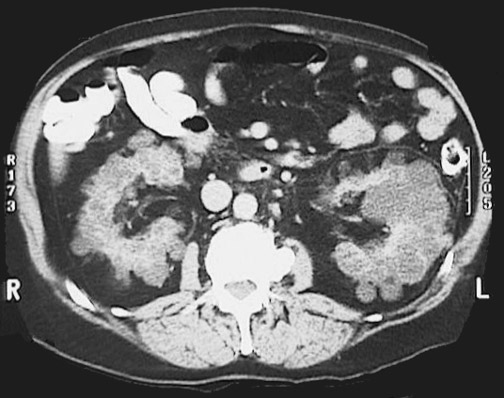
An abdominal CT shows markedly enlarged cystic kidneys bilaterally.
Questions:
7.1 What is suggested by these findings?
He has autosomal dominant polycystic kidney disease (ADPKD). Though there are inherited mutations in the polycystin 1 or 2 genes, the disease does not manifest itself until middle age, when the relentless development and enlargement of the renal cysts results in a reduction of functional renal parenchyma.
7.2 What pharmacologic therapy is indicated?
Hypertension occurs in over half of patients with ADPKD, even before the onset of renal failure. Activation of the renin-angiotensin-aldosterone system due to cyst expansion and local renal ischemia may occur in the development of hypertension in ADPKD. The combination of an angiotensin-converting enzyme (ACE) inhibitor along with an angiotensin receptor blocker (ARB) will be more effective than an ACE inhibitor alone.
Additional history:
Three years later, he has increasing malaise and decreasing urine volume. Laboratory studies show his serum creatinine is 5.6 mg/dL and urea nitrogen 68 mg/dL.
7.3 What should be done at this point?
He requires dialysis. Hemodialysis can be done on an ongoing basis. A renal biopsy is contra-indicated: there is a risk for rupture and hemorrhage of a cyst, and the diagnosis is obvious from an ultrasound or CT scan.
The dialysis machine for chronic hemodialysis requires venous and arterial access. On a long-term basis, a arteriovenous shunt is typically created in the forearm to facilitate this process. However, such a shunt increases cardiac output by about 10%, so persons who are in or who could develop congestive heart failure may not be candidates.
Dialysis is typically performed 3 times per week. The dialyzer is a plastic device with a semipermeable membrane through which the patient's blood passes on one side and the dialysate on the other side. The dialysate is an electrolyte solution adjusted to maintain and adjust the patient's electrolyte status while drawing off wastes. Each dialysis treatment uses about 120 L of dialysate with the following concentrations:
|
| | Sodium | 137 - 143 mmol/L
| | Potassium | 0 - 4.0 mmol/L
| | Chloride | 100 - 111 mmol/L
| | HCO3 | 30 - 35 mmol/L
| | Calcium | 0 - 3.5 mmol./L
| | Magnesium | 0.7 - 1.5 mmol/L
| | Acetate | 2 - 4.5 mmol/L
| | Glucose | 0 - 250 mg/dL
|
The concentrations of these substances can be adjusted during the procedure.
7.4 The patient is a jazz musician with no immediate family who travels frequently and whose income is quite variable through performances and CD sales. He wants to know how he will continue to receive treatment.
Hemodialysis in the U.S. is funded via the Medicare end-stage renal dialysis program, and the cost per patient per year is about $75,000. Dialysis centers are present in just about every major city in the U.S., so access is not typically a problem.
Of course, the ultimate solution is renal transplantation. He is on a list. Without relatives, he is at a slight disadvantage for donated kidneys from relatives, but regardless, relatives should not be pressured to donate.
7.5 How is drug therapy now affected?
Renal clearance is altered, and dialysis complicates dosing.
| 
