|
A 68-year-old woman has had increasing malaise for the past 6 years. On physical examination, vital signs include temperature 36.9 C, pulse 77/min, respiratory rate 16/min, and blood pressure 165/100 mm Hg. Laboratory studies show sodium 143 mmol/L, potassium 4.2 mmol/L, chloride 108 mmol/L, CO2 27 mmol/L, glucose 109 mg/dL, and urea nitrogen 40 mg/dL.
A 24 hour urine collection is performed.. There are 0.9 g of creatinine in 860 mL of urine. Her serum creatinine is 3.6 mg/dL.
Questions:
1.1 Calculate her creatinine clearance.
Urine creatinine x Urine volume in ml
Creatinine clearance = --------------------------------------
Plasma creatinine x time in min
105 mg/dL x 860 mL
= ---------------------------
3.6 mg/dL x 1440 min
= 17.4 mL/min
A "corrected" creatinine clearance can be calculated by multiplying by 1.73/total body surface area.
1.2 What does this indicate?
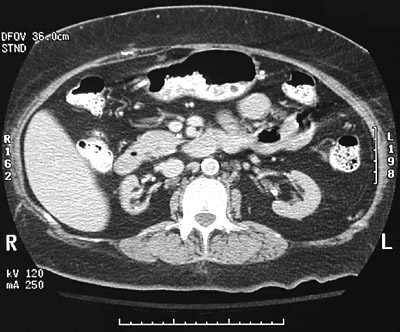
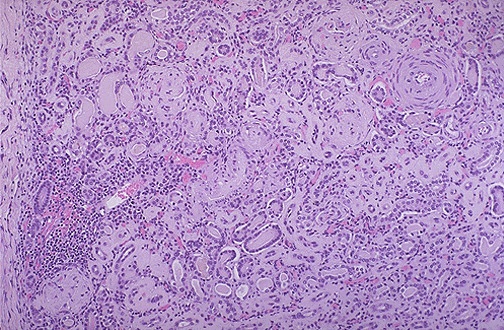
She has chronic renal failure with hypertension. The abdominal CT shows small kidneys with decreased parenchyma. The microscopic appearance is representative of "end stage renal disease" (ESRD) and often looks the same regardless of the underlying etiology, whether vascular, infectious, or immunologic in origin. With small, shrunken kidneys, a biopsy should NOT be done, because tissue is harder to obtain, and there is no useful information to be gained.
1.3 What pharmacologic therapy is indicated?
She should receive an angiotensin-converting enzyme (ACE) inhibitor and a loop diuretic such as furosemide. (Thiazide diuretics are ineffective when the creatinine clearance is <30 mL/min.) However, an ACE inhibitor should NOT be used when renal artery stenosis is present.
1.4 If she is receiving amoxicillin, how should the dose be adjusted?
Given that her renal function is compromised, the dose should be 1/3 the usual dose. (Note: the usual dose of amoxicillin for an adult is 500 mg t.i.d.)
| 
