Gastrointestinal Physiology
Return to the Main Menu
Case 1:
(Click here to go to the answers)
A 27-year-old woman has been bothered by bouts of abdominal pain, diarrhea, and constipation for the past 3 years. She has been a graduate student in biology for the past 3 years. On physical examination, vital signs show T 37 C, P 70/min, RR 15/min, and BP 95/65 mm Hg. She is in no distress. Her lungs are clear to auscultation and her heart rate is regular with no murmurs. There is mild abdominal tenderness on deep palpation of the epigastrium, but there are no masses and bowel sounds are present. A stool sample is negative for occult blood. The remainder of the examination is unremarkable. Laboratory studies show Hgb 14.8 g/dL, WBC count 7620/microliter, and platelet count 303,900/microliter. Her random blood glucose is 91 mg/dL, serum creatinine 1.0 mg/dL, and amylase 30 U/L. An abdominal ultrasound shows no abnormal findings.
Questions:
1.1 What should be considered?
Further history:
1.2 What is suggested by these findings?
1.3 What is the pathophysiology for this condition?
1.4 How is this condition treated?
Case 2:
(Click here to go to the answers)
A 70-year-old woman has had worsening fatigue with nausea and a 3 kg weight loss over the past year. On examination she is afebrile. Her heart rate is regular. There is no abdominal tenderness. The neurologic examination is unremarkable.
Laboratory studies show Hgb 11.8 g/dL, Hct 35.3%, MCV 85 fL, WBC count 5950/microliter, platelet count 229,300/microliter, sodium 141 mmol/L, potassium 4.0 mmol/L, chloride 104 mmol/L, HCO3 24 mmol/L, glucose 72 mg/dL, creatinine 0.7 mg/dL, total protein 5.6 g/dL, albumin 3.4 g/dL, LDH 510 U/L, alkaline phosphatase 61 U/L, AST 281 U/L, ALT 307 U/L, total bilirubin 4.8 mg/dL, and direct bilirubin 3.0 mg/dL.
Questions:
2.1 What is suggested by these findings?
2.2 What additional laboratory tests are indicated?
Additional laboratory studies show:
| HBsAg | negative
| | HBsAb | positive
| | HBcAb | negative
| | HCVab | positive
| | HAV-IgM | negative
| | HAV-IgG | positive
|
2.3 What do these findings indicate?
2.4 Explain the pathophysiology of the liver function tests.
2.5 How should she be treated?
2.6 What dietary modifications may be useful for this patient if hepatic function worsens?
Case 3:
(Click here to go to the answers)
A 34-year-old woman has noted intermittent but sharp abdominal pains for the past 2 days. On physical examination her vital signs include T 37 C, P 83/min, RR 18/min, and BP 140/90 mm Hg. Her lungs are clear to auscultation and her heart rate is regular with no murmurs. She has right upper quadrant tenderness on palpation. Bowel sounds are active. Her stool has no detectable occult blood. Laboratory studies show Hgb 11.8 g/dL, Hct 36.0%, MCV 121 fL, WBC count 9200/microliter, platelet count 262,000/microliter, glucose 66 mg/dL, creatinine 0.9 mg/dL, amylase 22 U/L, AST 44 U/L, ALT 25 U/L, total bilirubin 1.0 mg/dL, and alkaline phosphatase 69 U/L.
Questions:
3.1 What do you suspect and what studies would you perform?
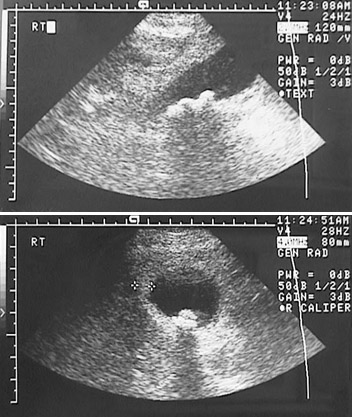
Additional history:
She has had bouts of abdominal pain for the past 7 years. These bouts have lasted from 1 to 4 weeks on average, accompanied by diarrhea.
3.2 What is suggested by these findings?
An abdominal CT scan is performed:
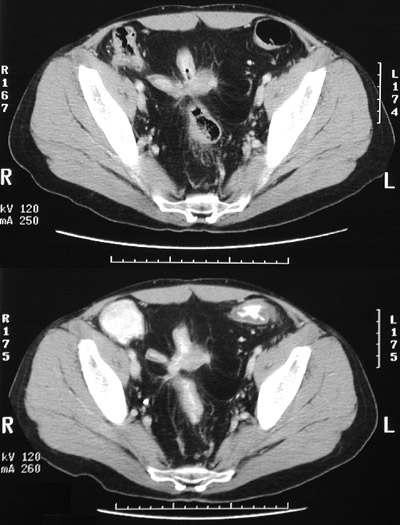
3.3 How does this explain the initial findings above?
3.4 What if this patient's total bilirubin had been 3 mg/dL? Explain bilirubin metabolism.
Case 4:
(Click here to go to the answers)
A 51-year-old man has been bothered by chest pain for the past 20 years. He describes the pain as dull and burning. On physical examination there are no abnormal findings. Upper GI endoscopy shows the findings seen here:
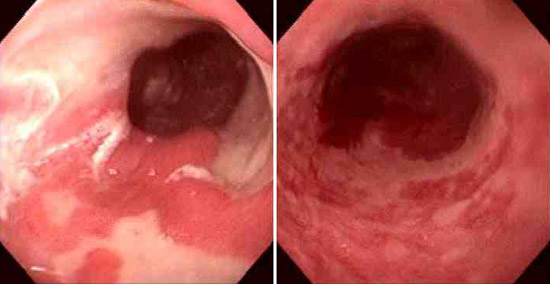
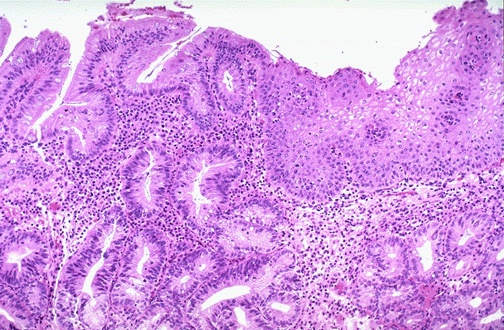
A biopsy shows the microscopic finding seen here:
Questions:
4.1 What is the diagnosis?
4.2 What is the pathophysiology of this condition? What condition is the opposite of this one?
4.3 What pharmacologic therapy is available? How does it work?
Case 5:
(Click here to go to the answers)
A 77-year-old woman comes to her physician for a routine checkup. Her only problem on review of systems is chronic constipation. The physical examination is unremarkable.
Questions:
5.1 Explain potential causes for this condition.
5.2 What should be done?
5.3 What treatment plans are useful?
5.4 Describe normal gastrointestinal motility.
5.5 What causes ileus?
5.6 History of medicine.
Case 6:
(Click here to go to the answers)
A 10-month-old infant is noted by his mother to have had more frequent, watery stools over the past 2 days. On examination vital signs include T 37.2 C, P 103/min, RR 12/min, and BP 85/45 mm Hg. The child is listless and has poor skin turgor. The child is at the 45th percentile for weight and the 55th percentile for height. No congenital abnormalities are noted. Laboratory studies show Hgb 16.2 g/dL, Hct 49.2%, MCV 95 fL, platelet count 188,700/microliter, and WBC count 7770/microliter. Serum electrolytes include sodium 159 mmol/L, potassium 3.6 mmol/L, chloride 125 mmol/L, CO2 18 mmol/L, glucose 62 mg/dL, creatinine 0.4 mg/dL, and bilirubin 0.7 mg/dL.
Questions:
6.1 What is suggested by these findings?
6.2 What are possible etiologies for this condition?
6.3 What therapies can be employed?
6.4 Describe the physiology of gastrointestinal water and electrolyte absorption in adults.
6.5 Describe the acid-base disturbances that result from: 1) prolonged vomiting; 2) prolonged diarrhea.
Case 7:
(Click here to go to the answers)
A 35-year-old man has had diarrhea with a 5 kg weight loss over the past year. On physical examination there are no abnormal findings. Laboratory studies show Hgb 13.5 g/dL, Hct 40.6%, MCV 89 fL, platelet count 241,000/microliter, WBC count 5580/microliter, sodium 142 mmol/L, potassium 4.0 mmol/L, chloride 110 mmol/L, CO2 22 mmol/L, glucose 72 mg/dL, creatinine 0.9 mg/dL, amylase 30 U/L, total protein 5.8 g/dL, albumin 3.7 g/dL, AST 28 U/L, ALT 19 U/L, alkaline phosphatase 77 U/L, and total bilirubin 1.0 mg/dL.
Questions:
7.1 What diagnoses may be considered?
7.2 What else do you want to know?
7.3 What diagnostic tests can be done?
Upper GI endoscopy is performed. There are no esophageal or gastric lesions; duodenum shows slight erythema; jejunum shows loss of mucosal folds and erythema.
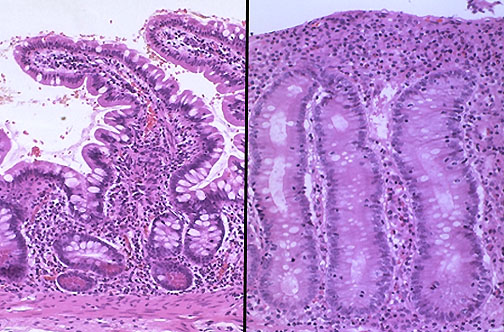
Jejunal biopsy has the microscopic appearance shown at the right (compared with normal at the left), with loss of villi, flattening of villi, increased inflammation, and diminished goblet cells.
7.4 What is the diagnosis?
7.5 What is the cause for this? What is the mechanism for the diarrhea?
7.6 What is the treatment?
7.7 What are complications?
7.8 Outline the absorption mechanisms for carbohydrates, fats, and proteins.
Case 8:
(Click here to go to the answers)
In 1631, during the Thirty Years War, the city of Rothenburg-ob-der Tauber was besieged and captured by Catholic forces under the command of Johan Tzerclaes von Tilly. He threatened to execute the city councilors and destroy the city. At that moment, the Pokal, a huge ceremonial container, was then filled to the brim with the city's best wine. This drinking vessel, which held three liters, was passed around and around in celebration by General Tilly and his staff, but some wine remained, even after repeated rounds of drinking. It was then the General decided on a whim to spare the city if one Rothenburger could drink in one draught the contents of the Pokal, and who would be willing to do so, knowing that the wine was poisoned. The former mayor, Georg Nusch, accepted the challenge and downed the three liters of wine. He then passed out and slept for three days, but survived. (Note: the wine was not poisoned, since no one would have wanted to ruin the wine and have it left over had the challenge failed).
Questions:
8.1 What is the absorption and distribution of ethanol?
8.2 If the standard German Riesling (a white wine) is 12% alcohol by volume, what would be Mayor Nusch's blood alcohol an hour following the challenge? Calculate values for a standard 70 kg man, an athletic 90 kg man, and a corpulent 110 kg man.
8.3 What would his blood alcohol level be a day later?
Return to the Main Menu
|