Endocrine/Reproductive Physiology
Return to the Main Menu
Case 1:
(Click here to go to the answers)
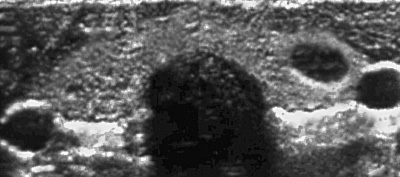
A 43-year-old previously healthy woman has a routine medical checkup. Her physician palpates a firm nodule in her left neck region. An ultrasound scan reveals the following:
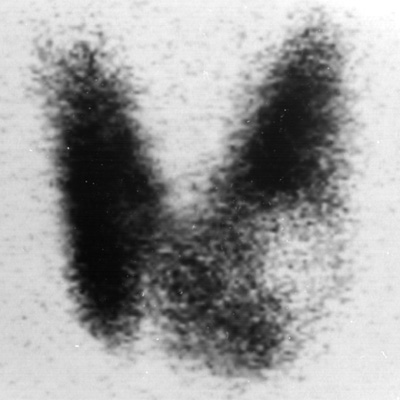
A radionuclide scan reveals the following:
A fine needle aspirate of the nodule is performed. She then undergoes thyroidectomy with the finding seen below:

Questions:
1.1 What is the diagnosis?
1.2 What testing is required in the immediate post-operative period? Hint: what is shown in the EKG below?
1.3 What long-term complication should be monitored?
1.4 What therapy is indicated?
1.5 How do hormones affect their targets?
Case 2:
(Click here to go to the answers)
A 24-year-old woman is in the third trimester of her first pregnancy. There have been no problems, with fundal height consistent for gestational age. She goes into labor and begins hemorrhaging profusely. She is taken to the hospital, and on admission has vital signs with T 36.8 C, P 116/min, RR 22/min, and BP 80/40 mm Hg. Her skin is cool and clammy. She has marked vaginal bleeding. An abdominal ultrasound shows a low-lying placenta. The fetus is viable, with heart tones from 140 to 150/min. Laboratory studies show Hgb 6.4 g/dL, Hct 19%, MCV 80 fL, platelet count 207,300/microliter, and WBC count 5920/microliter.
Questions:
2.1 What is the diagnosis?
2.2 What should be done next?
Additional history:
A month following delivery she is unable to nurse the baby. She has increasing polyuria and polydipsia. She then has a fainting episode. MR imaging of the head reveals the following:
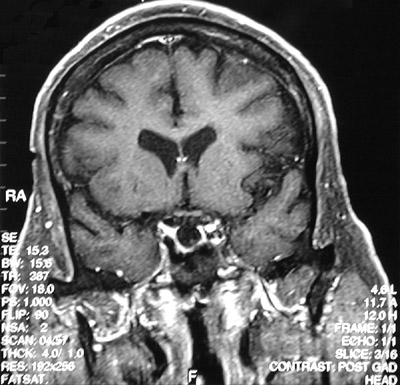
2.3 Explain these findings.
Laboratory studies show Hct 30%, sodium 129 mmol/L, potassium 5.0 mmol/L, chloride 89 mmol/L, CO2 19 mmol/L, glucose 60 mg/dL, and creatinine 1.0 mg/dL.
2.4 If she is not treated at this point, what could happen?
2.5 What is the treatment?
Case 3:
(Click here to go to the answers)
A 41-year-old chief executive officer of a corporation has noted increasing thirst over the past 3 months. His fluid consumption has increased, and he is spending more time in rest rooms, which interferes with business meetings. He has not seen a physician for the past 20 years, since discharge from military service. On physical examination his temperature is 37 C, pulse 74/min, respiratory rate 16/min, and blood pressure 140/85 mm Hg. He has decreased sensation to light touch and pinprick in his lower extremities. He has decreased range of movement with crepitus and pain in his knees bilaterally. His BMI is 31.
Laboratory studies show Hgb 13.5 g/dL, Hct 40.7%, MCV 90 fL, platelet count 263,700/microliter, WBC count 8330/microliter, sodium 143 mmol/L, potassium 4.2 mmol/L, chloride 108 mmol/L, CO2 26 mmol/L, glucose 155 mg/dL, creatinine 1.2 mg/dL, total protein 5.8 g/dL, albumin 4 g/dL, and total bilirubin 0.9 mg/dL. A urinalysis shows pH 7, sp gr 1.015, glucose 2+, protein 1+, blood negative, and ketones negative.
Questions:
3.1 What is suggested by these findings?
3.2 What therapy is indicated?
3.3 How would your assess this patient's compliance or adherence with his diabetes treatment?
3.4 You ask the patient to bring in his oral medication and conduct a pill count. He appears to be taking all of his medication as prescribed. You also contact the patient's pharmacy and learn that he has been refilling his prescription on a regular basis. Would you describe this patient as a "compliant" patient?
Case 4:
(Click here to go to the answers)
A 13-year-old girl has been observed by her parents to be eating and drinking a lot of junk food and carbonated beverages for the past 2 months. In spite of this diet she appears to be getting thinner. Her mother takes her to the physician. On physical examination her temperature is 37 C, pulse 74/min, respiratory rate 20/min, and blood pressure 90/60 mm Hg. She has peripheral muscle wasting. She is 165 cm tall and weighs 47 kg.
Laboratory studies show Hgb 13.2 g/dL, Hct 40%, MCV 94 fL, platelet count 290,200/microliter, WBC count 6990/microliter, sodium 149 mmol/L, potassium 4.9 mmol/L, chloride 113 mmol/L, CO2 9 mmol/L, glucose 394 mg/dL, creatinine 0.7 mg/dL, total protein 6.2 g/dL, albumin 4 g/dL, and total bilirubin 1.1 mg/dL. A urinalysis shows pH 6, sp gr 1.011, glucose 4+, protein negative, blood negative, and ketones 4+.
Questions:
4.1 What is the diagnosis?
4.2 What therapy is indicated?
4.3 She is poorly adherent to therapy. She eats whatever she wants. What options can be employed? Her Hgb A1C is still only 5.8%. Why is this possible?
4.4 What kinds of information would you gather or what assessments would you conduct to advise this young woman and her family about her diet?
Case 5:
(Click here to go to the answers)
A 37-year-old woman has noted loss of normal menstrual cycles in the past 6 months and increased growth of body hair. On physical examination her temperature is 37 C, pulse 70/min, respiratory rate 15/min, and blood pressure 145/95 mm Hg. Her motor strength is 4/5 in all extremities. She has fat redistribution centrally. Her body mass index is 33.
Questions:
5.1 What are possible causes?
5.2 What additional studies are needed?
5.3 What radiographic findings do you expect?

5.4 What is the diagnosis?
Case 6:
(Click here to go to the answers)
A 38-year-old woman and her 47-year-old husband are trying to have a child. This is the 2nd marriage for both of them. She has 1 child and he has 2 children by former marriages. They remarried 13 months ago.
The wife has been surfing the internet for information about in-vitro fertilization (IVF). She has come across several fertility clinics that make it all sound so easy: "Take home a baby or we will refund 70% of your money-No risk!" She is overly optimistic that they will be able to have a baby with these methods.
Questions:
6.1 What should the physician take into consideration when talking to the couple about their chances of having a baby with IVF?
6.2 What conditions should be considered before jumping directly to IVF?
Additional history:
On physical examination, she is 162 cm tall and weighs 65.6 kg. Her vital signs are: T 38.1 C, P 105/min, RR 20/min, and BP 140/80 mm Hg. There are no remarkable findings except for a fine tremor of her outstreched hands. Review of systems reveals that she has been trying to lose weight over the past year, and has lost 4 kg. She has been bothered by occasional diarrhea during the past year.
On physical examination, he is 178 cm tall and weighs 95 kg. His vital signs are: T 37 C, P 79/min, RR 15/min, and BP 135/85 mm Hg. There are no major findings on physical examination. An orchidometer is used to estimate the testicular volume, which is greater than 20 cc on the right and <20 cc on the left. Review of systems reveals that he has had exertional angina for the past 3 years, for which he was prescribed a "heart pill".
6.3 What do you make of these findings?
The man does not, of course, have the "heart pills" with him, so he calls you upon returning home and looking at the bottle and reading off, "d-i-l-t-i-a-z-e-m." ®
6.4 What should you do next?
Additional history:
After 6 more months, she has had short or irregular menstrual cycles. He feels as though he has more energy.
6.5 How could you tell if she is going through menopause? What do you do next?
Have you forgotten about him? Have we gotten a sperm count with morphology yet? His sperm count is 3 million, with >95% motile, morphologically normal sperm.
6.6 What can you do next?
Case 7:
(Click here to go to the answers)
A 15-year-old boy is brought to the physician by his parents who are concerned about his development. The boy feels ostracized by classmates at school, who tease him because of his small size. He dreads physical education classes. The other boys have more development of secondary sexual characteristics. He has been an above average student through grade school, but is now performing at just an average level.
Questions:
7.1 Review normal development.
SMR Pubic Hair Stages: Mean chronologic age (CA) and bone age (BA)
in males and females (in years)
| SMR | Male CA | Male BA | Female CA | Female BA
| | I. None
| | II. Sparse | 12.2 | 13.5 | 10.4 | 11.5
| | III. Coarse, easily visible | 13.5 | 14.2 | 12.2 | 12.2
| | IV. Confined to suprapubic area | 14.2 | 14.2 | 13.0 | 13.2
| | V. Adult type on medial thighs | 14.9 | 14.0
|
Stage II-V = 2.7 yrs avg.
SMR Female Breast Stages: Mean chronologic age (CA) and bone age (BA)in females (in years)
| SMR | CA | BA
| | I. No development
| | II. Bud | 10.9 (8.5-13.3) | 10.5
| | III. Breast tissue beyond areola | 12.2 | 12.0
| | IV. Secondary mound | 13.2 | 13.5
| | V. Adult | 14.0 | 15.0
| | Peak height velocity | 12.2 (10.2-14.2) | 12.5
| | Menarche | 12.7 (10.5-15.5)
|
Stage II to Stage III = 1.3 yrs avg.
Stage III to Stage V = 2.4 yrs avg.
SMR Male Genital Stages. Mean chronologic age (CA) and bone age (BA)
in males (in years)
| SMR | Testicular Length | Testicular Volume | CA | BA
| | I. | <2.5cm | <4ml
| | II. | >2.5cm | 4-6 ml | 11.2 (9.2-14.2) | 11.5 (9.0-13.5)
| | III. | >3.0cm | 6-10 ml | 12.9 | 13.2
| | IV. | >4.0cm | 10-15 ml | 13.8 | 14.5
| | V. | >5.0cm | >15ml | 14.7
| | Peak height velocity | | | 13.9 (12.3-15.5) | 14.5
|
Females initially show a deposition of adipose tissue and widening of the pelvis and changes in the contour of the hips. The first clinical sign is thelarche (the appearance of breast buds) and adrenarche (the appearance of dark straight pubic hair over the mons veneris, also called the mons pubis). These changes identify a SMR stage (or Tanner stage) II (see tables 1 and 2). Breast development over the next 4 years will proceed from breast stage II (secondary mound of breast tissue to adult breast stage V). Development of pubic hair starts about 1 year after breast budding and may take place over a 1.5 to 3.5 year period. During SMR stage 3, girls experience a very rapid increase in their height. The peak of their height growth (PHV=peak height velocity) should take place before the onset of menarche in most girls. Menarche occurs six months after the PHV and just prior to stage IV of breast development. Most western girls achieve their menarche around 12.4 to 12.8 years of age. African-American girls are maturing earlier.
Puberty in boys also follows a regular sequence of events, but lacks the clear cut landmarks such as breast development and menarche. In the male, the pubertal growth spurt is a late event starting about two years later than in females. The onset of pubertal changes however, are only about 6 months later than in females (see tables 2 and 3). Enlargement of the testes indicates the transition from genital stage I to Stage II, beginning at an average age of 11.5 years. Penile growth occurs about one year later. This is usually preceded by the appearance of pubic hair at the base of the phallus progressing through pubic hair stages II to V. Pubic hair stage III is followed by the appearance of axillary and facial hair growth. Testicular growth is completed anytime between 13.5 and 17 years of age. Growth of the penis reaches a SMR (Tanner) stage V between 12.5 and 16.5 years of age. Nocturnal emissions (wet dreams) may first appear during SMR stage III.
Additional history
Past History: He was the product of a normal term gestation. He weighed 4 kg at birth with normal height (52 cm) and head circumference (35 cm). He met developmental milestones during infancy and childhood. He has had no major medical problems. He takes no medications.
Family History: His mother is 33 years old and in good health. Her height is 175 cm and her weight is 70 kg. She had menarche began at age 13. His father is 36 years old, also in good health. His height is 190 cm and his weight is 90 kg. He remembers having a "growth spurt" at age 12. The boy has a 14-year-old sibling, a sister, who is 165 cm tall and weighs 55 kg. She started menarche at age 12.
Physical examination shows vital signs with T 37 C, P 80/min, RR 19/min, and BP 95/65 mm Hg. His current height is 147 cm and his weight is 41 kg. He appears normally proportioned and there are no apparent congenital anomalies. On auscultation of the chest his heart rate is regular with no murmurs and his lungs are clear. Palpation of his abdomen reveals no masses, and on auscultation bowel sounds are present. Pulses are 2+ and motor strength 5/5 in all extremities. The neurologic examination is unremarkable. The genital exam shows a normal circumcised penis. His Tanner pubic hair stage is 1, with genital stage 2. The scrotum has a normal midline raphe. Both testes are palpable in the scrotum, each with estimated 4 mL in volume by measurement with an orchidometer. His testes are firm, 2.5 cm in length and 4 ml in volume.
Laboratory findings include Hgb 13.7 g/dL, Hct 41.3%, MCV 90 fL, platelet count 199,000/microliter, and WBC count 7160/microliter. His serum sodium is 143 mmol/L, potassium 4.1 mmol/L, chloride 105 mmol/L, CO2 26 mmol/L, glucose 74 mg/dL, and creatinine 0.7 mg/dL. A urinalysis shows pH 6.5, sp gr 1.020, and no blood, protein, glucose, or ketones.
7.2 What is suggested by these findings?
7.3 What additional studies can be performed?
7.4 What is your diagnosis?
7.5 The parents have seen cases like this on television shows, and those children received treatments that made them "normal". The parents want you to do something.
Additional History: On a return visit, the boy now has growth of pubic hair and his testicular volume has increased. His height is 153 cm and weight 45 kg.
Clinical Course: Over the next 6 months, pubic hair growth is noted. His testes enlarge to 3-4 cm in length and his height increases by 5 cm.
7.6 What would be your diagnosis if the laboratory value in 7.3 had been lower?
Return to the Main Menu
|