|
A 30-year-old injection drug user develops a high fever and chills. On examination vital signs show temperature 39.2 C, pulse 115/min, respiratory rate 20/min, and blood pressure 80/50 mm Hg. Auscultation of the chest reveals a holosystolic murmur at the lower left sternal border. The intensity of the murmur increases with inspiration. Observation of the neck veins reveals the following venous pulsations
Questions:
9.1 What do these findings indicate?
He has tricuspid regurgitation. This is likely due to acute bacterial endocarditis.
9.2 What additional studies should you do?
Blood culture. The culture grows Pseudomonas aeruginosa.
Additional history:
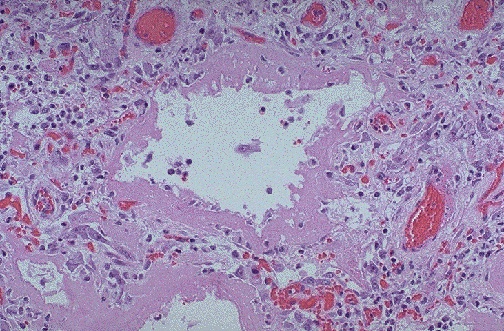
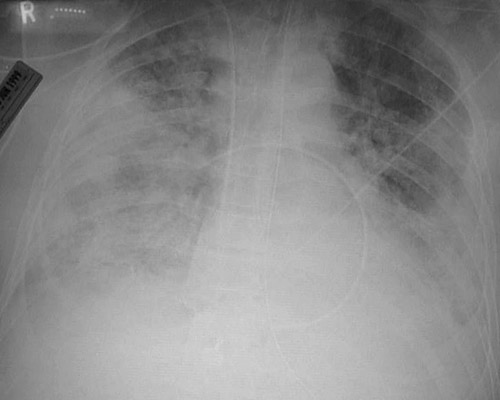
He undergoes emergent surgery with tricuspid valve replacement. He receives antibiotic therapy with ticaracillin and tobramycin. A repeat blood culture shows no growth. He requires supplemental oxygen with an FI02 of .80. Examination of the lungs shows crackles bilaterally. He has tachycardia without an S3 gallop. Chest roentgenogram reveals diffuse infiltrates in both lung fields with an alveolar pattern.
He now has the following hemodynamic pressure measurements:
| Arterial BP | 105/70 mm Hg
| | RA (CVP) | 8 mm Hg
| | PA | 60/32 mm Hg
| | PAWP | 10 mm Hg
| | HR | 106/min
|
9.3 What is suggested by these findings?
An acute restrictive lung disease, typical for diffuse alveolar damage (clinically known as adult respiratory distress syndrome) can produce this markedly elevated pulmonary arterial pressure.
9.4 If his left chamber volume at end of diastole = 0.12 L, chamber volume at end of systole = 0.07 L, and he is an average-sized person with a body surface area of 1.62 m2, calculate his cardiac output, cardiac index, and ejection fraction.
Stroke Volume = ((Chamber Volume at End Diastole) - (Chamber Volume at End Systole)) = 0.05 L
Cardiac Output = (Stroke Volume) X (Heart Rate) = 5.3 L/min
Cardiac Index = (Cardiac Output) / (Body Surface Area) = 3.27 L/min/m2
Ejection Fraction = ((Stroke Volume) / (Chamber Volume at End Diastole)) * 100 = 42%
9.5 What is DLCO and what would you expect it to be in this case?
The DLCO is a measure of pulmonary diffusing capacity. It is measured by having the patient inhale air containing 0.3% carbon monoxide, holding the breath for about 10 seconds, and then measuring the CO in the exhaled breath. The DLCO is calculated as the amount of CO absorbed per minute per A-a gradient.
The DLCO is affected by diffusion blocks (thickness of the alveolar-capillary membrane, V/Q mismatches, alveolar-capillary surface area, and the hemoglobin). Usually, the DLCO is adjusted for the hemoglobin.
Diseases that affect only airways (such as chronic bronchitis or upper airway obstruction) do not affect the DLCO. Diseases that affect the alveolar walls (DAD or emphysema) or the pulmonary capillary bed (thromboembolism or vasculitis) will decrease the DLCO.
| 
